Presented by: Tom L. Rosamond, MD, MSc, FAHA, FACC, FASE
Dr. Thomas Rosamond is Board Certified in Cardiovascular Disease. Dr. Rosamond is the Division Chief of Cardiovascular Imaging and Medical Director of Non-Invasive Imaging Services at The University of Kansas Health System. He earned his Postdoctoral Fellowship in Cardiovascular Magnetic Resonance Imaging at Washington University School of Medicine -Barnes Jewish Hospital in St. Louis, Missouri.
Systemic Sclerosis Case Study: Cardiac Imaging Findings
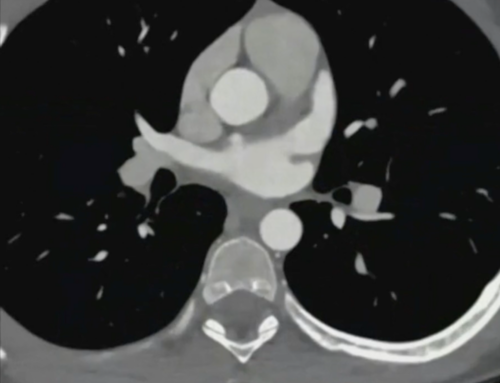
Systemic sclerosis, also known as scleroderma, is an autoimmune disorder that can affect multiple organ systems, including the lungs, heart, and musculoskeletal system. Dr. Tom Rosamond, division chief of advanced cardiovascular imaging at the University of Kansas Health System, presents the case of a 63-year-old female patient with systemic sclerosis affecting the pulmonary, cardiac, and skeletal systems.
Patient History
The patient presented with dyspnea and underwent a coronary angiogram and Resting Full-cycle Ratio (RFR) correlation.
Angiogram and RFR Findings
The coronary angiogram showed modest coronary stenosis, with 50% stenosis in the ostium and mid-segment of the Left Anterior Descending (LAD) artery. The left circumflex artery was non-dominant, and the right coronary artery had a 3% modest stenosis. The RFR results indicated hemodynamically significant areas in the distal LAD, with equivocation in the mid and proximal LAD.
Ammonia PET Scan
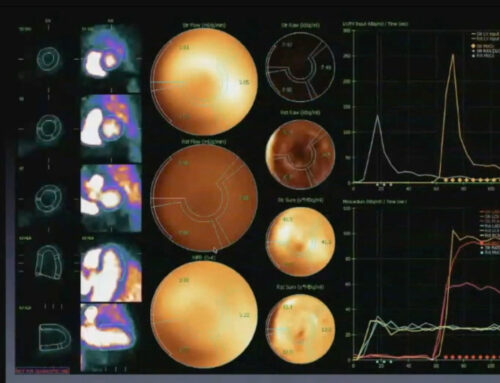
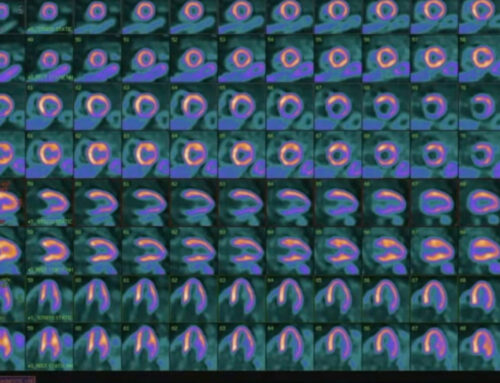
To further evaluate the patient, an ammonia PET scan was performed. The key findings were:
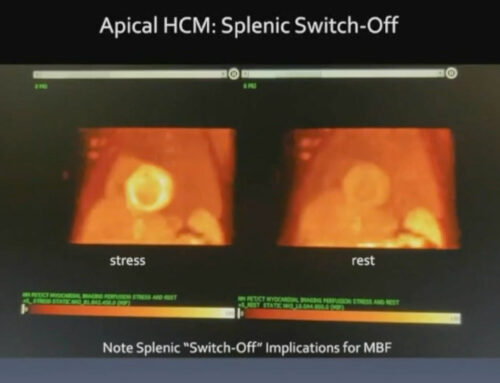
- Presence of an apical defect on the stress images
- Normal left ventricular function, with an ejection fraction of 82% at rest and 78% at stress
- Quantification data showed a small affected area, comprising 3% of the left ventricular myocardium at stress and 1% at rest
Flow Data Analysis
Analysis of the flow data demonstrated diminished flow in the LAD compared to the other coronary arteries. Segmental analysis revealed the apical defect had a stress flow of 1.84, compared to 2-3 in the other segments.
Conclusion and Recommendation
Dr. Rosamond concluded that the case represented a distal LAD mild intensity, small reversible defect with low risk. He recommended medical management rather than coronary intervention, emphasizing that stenting is not necessary for a 30-40% stenosis despite positive RFR results.